Studying the Whole Spectrum
Autism research often excludes those who stand to benefit most
Image Credit: Tara Holley
By Romila Santra
December 6, 2022
My twin brother Rohan prances around the house — first to the pantry to investigate snacks, then to the TV blaring “Winnie the Pooh,” then to the dining table to pick at the pomegranate seeds my mom puts out for him. At 20, he functions like a child one-tenth his age. He uses modified sign language but cannot speak a word, and he distinguishes between sarcasm and sincerity but cannot regulate emotions. His autism diagnosis arrived when we were toddlers and never left, irreparably splitting our developmental paths.
Since I’m a research coordinator in a neurodevelopmental lab studying children with autism, you might think I work with kids like Rohan frequently. I don’t.
Impaired social communication and restricted, repetitive behaviors define autism spectrum disorder. The “spectrum” characterizes autism’s range of causes, symptoms, and severity. This range is so expansive that Stephen Shore, an autistic professor of special education at Adelphi University, famously said, “If you’ve met one person with autism, you’ve met one person with autism.”
The children at my lab cluster at the lower support needs end of the spectrum. Though they may struggle with social awkwardness, overstimulation, and behavioral outbursts, they — unlike my brother — will likely grow up to live independent lives.
About 30% of kids with autism have an intellectual disability or are minimally verbal. Yet, a 2017 review found that only 11% of research participants fit that profile. Unfortunately, excluding severely autistic children from research means we risk misunderstanding the complexity of the disorder. It also means our work overlooks those who would benefit most from earlier therapies and experimental treatments.
As a family member and researcher, I’m acutely aware of the logistical challenges of working with severely autistic children. It takes only one look at a visit schedule with our 8- to 12-year-old subjects to understand why.
9:30 a.m.: Consent
A guardian, the child, and I gather in a loose triangle, a stack of paperwork in my lap. We run through the child’s rights as a participant, the day’s activities, and their concerns. While the guardian provides the “big-C” consent, the child provides assent, signaling willingness to participate.
For a severely autistic child like Rohan, our parents would have to make the call (he has no concept of time, let alone scientific research, and can’t sign his name). Is it acceptable to enroll participants like him without informed consent or even assent?
The institutional review board approves study designs, protects the welfare of research subjects, and serves as final arbiter in ethical gray areas. There’s no handbook, only best practices derived from years of human research. As with other cognitively impaired patients, consent must be ongoing throughout the study. Even low support needs kids might withdraw their morning assent for an MRI upon experiencing overwhelming anxiety or claustrophobia in the scanner.
10 a.m.-12 p.m.: IQ testing
Participants spend two hours with our psychologist to undergo cognitive testing. If the child demonstrates an intellectual disability, they are disqualified.
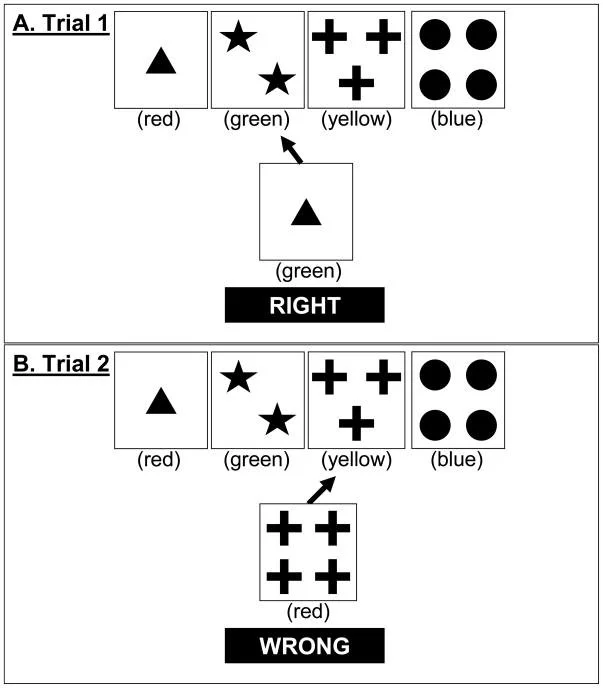
The Wisconsin Card Sorting Test (WCST) asks study participants to sort and pair cards which vary in color, shape type, or number of shapes. After a set number of rounds the experimenter changes the grouping criteria, only telling the participant if the new pairing is correct or not correct. Recognizing this shift in testing criteria is an indicator of cognitive flexibility. Image credit: National Institutes of Health.
Though about one-third of autistic children have IQs in the intellectual disability range, our lab is not alone in using this exclusion criterion. A 2019 meta-analysis from researchers in the U.K. examined 301 studies and found only 6% of autistic participants had an intellectual disability. Most study tasks required minimal comprehension, disqualifying many participants. For example, a handwriting assessment means children must read, write, and understand instructions — my brother can’t even hold a pencil. Even an MRI scan involves directions.
Although many research groups don’t design tasks for children with low comprehension, some have begun to modify existing paradigms. Some researchers balance data collection to account for longer processing speeds and lower mental ages — tasks must be shorter, more colorful, and disguised as play.
Take the Wisconsin Card Sorting Test, used since 1948 to ascertain mental flexibility. The original version involves 128 cards printed with various shapes, numbers, and colors. In 2011, researchers in the U.K. and Italy set out to study flexibility in children with autism who have low support needs. They pared 128 cards down to 16, and instead of shapes, colors, and numbers, they used only shapes and colors. Simplifying this well-known task allowed them to collect solid data from this poorly studied population.
1-3 p.m.: Computer tasks and other testing
The post-lunch slump features an onerous, 50-year-old test of impulsiveness. A screen flashes one of two stimuli: one for which participants must quickly press a button and another for which they must not. We tell the kids they’ve “arrived at the U.S. Space Command!” But no thrilling pretense dulls 20 minutes of pushing the space bar in response to green spaceships and not pressing for red spaceships. “I’m going to leave a bad review for these games when I go home!” one disgruntled subject told me.
Tasks like these push participants who need low support to their limits. Rohan would be out of his seat within two minutes.
3:30-4:30 p.m.: MRI
Our scanner is a beige behemoth that fills an entire room. To get a brain scan, a child lies on a plastic board and is rolled into a small opening. Then comes the hard part: bombardment with beeps as loud as air horn blasts — a challenge for anyone, but especially for autistic individuals sensitive to sensory input. Even in our well-oiled lab with experienced staff, it’s a coin toss as to whether we’ll get usable scans.
To help kids acclimate to an MRI, we often schedule a mock scan in a decommissioned machine. Children with severe autism often need more practice to become comfortable. A single scan costs about a thousand dollars of hard-earned funding. It’s an expensive gamble that requires one crucial thing: a still body. That’s a huge ask for any kid, let alone those on the spectrum.
Luckily, a new technique called functional near-infrared spectroscopy, or fNIRS, might soon make waves in autism research. The fNIRS setup looks like a black, polka-dotted swim cap with a chinstrap, but its hidden beauty lies in how portable, cheap, quiet, and motion-tolerant it is. Theoretically, a wiggly child could produce usable data. While the resulting images aren’t as fine-grained as an MRI, they’re resolute enough to identify regional brain activity differences due to autism.
4:30-5:30 p.m.: The day ends
After the kids leave and I enter their data, I’m left to ponder how far the field of autism research has come and how very far we have to go.
Though broader inclusion demands a more robust investment of money and time, the endeavor is not only worthwhile, it is necessary. A 2017 analysis describing the lack of people with high support needs representation in autism research noted that “extensive planning with family, experienced staff, and thoughtful experimental design” can make a difference. Asking guardians about their child’s unique needs yields critical nuggets of information: Do visual schedules or timers help transitions? Should bathroom breaks be prompted? Are there particular topics of conversation they enjoy?
My concerns stem from my role as both a researcher and a sister. If one-third of autistic children aren’t represented in studies, how are they to reap the benefits of our best science?

Romila Santra
Romila Santra is a graduate student in the Johns Hopkins University Science Writing Program. Before joining the program, she graduated with neuroscience and medical humanities degrees, also from Johns Hopkins. She is applying to medical schools with the hope of eventually becoming a physician-writer. In her free time, Romila enjoys running the “Secret Life of Sibs” podcast, watching her favorite sitcoms, and baking.